Lateral or pain on the outside of the elbow is an extremely common complaint we see in our Melbourne City sports chiropractic clinic. In lay terms it is referred to as �tennis elbow� or �epicondylitis� however as Melbourne sports...
Lateral or pain on the outside of the elbow is an extremely common complaint we see in our Melbourne City sports chiropractic clinic. In lay terms it is referred to as �tennis elbow� or �epicondylitis� however as Melbourne sports chiropractor Dr. Shannon explains in his article for the Australian Chiropractic Magazine below, these terms are outdated and should be replaced with the more appropriate term �lateral elbow tendinopathy.�
Patients with tendon pain present with impaired function and a decreased tolerance for exercise which becomes a challenge not only for the patient but also for the clinician. Tendon pathology more commonly occurs at the tendon bone attachment site such as in the elbow but, can also occur in the mid-tendon as seen in the achilles. Regardless of the location, the pathological changes that occur in the tendon appear the same (1).
Why Tendons Cause Pain
Tendons are responsible for capturing and releasing energy and this is done primarily through a well organised tendon cell structure and via type 1 collagen fibres (2). When excessive load is put through a tendon it leads to cell breakdown.
This process of cellular breakdown includes apoptosis (programmed cell death), destruction of the cell matrix, disorganisation of the collagen fibre arrangement and changes in the quality of collagen fibres with an increase in type III collagen, neovascularisation (infiltration of new blood and nerve vessels), along with an increase in fatty tissue, proteoglycans and tenocytes (1,3�6).
This cell structure breakdown correlates with the clinical signs and symptoms often associated with tendon pathology such as; tendon thickening as a result of proteoglycans retaining fluid and pain which is thought to be caused by neovascularisation. Together the cell breakdown ultimately affects the tendon�s inability to carry out its function to capture and release energy, leading to a dysfunctional and degenerative tendon.
Tendon Pain Continuum
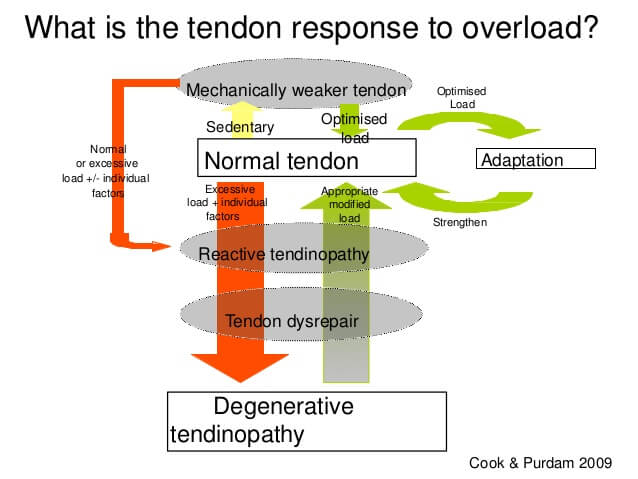
It is currently proposed that tendon pathology occurs along a 3 stage continuum where tendon overload drives tendon breakdown along the continuum from a reactive tendon, to tendon disrepair (failed healing) and finally to a degenerative tendon (1). Early in the continuum reversibility of the tendon pathology is possible however, this becomes unlikely in the degenerative stage.� Adding or removing tendon load is the primary stimulus that drives tendon change forward and backwards along the continuum in the early stages (1).
How Tendon Loading Impacts Tendon Pain
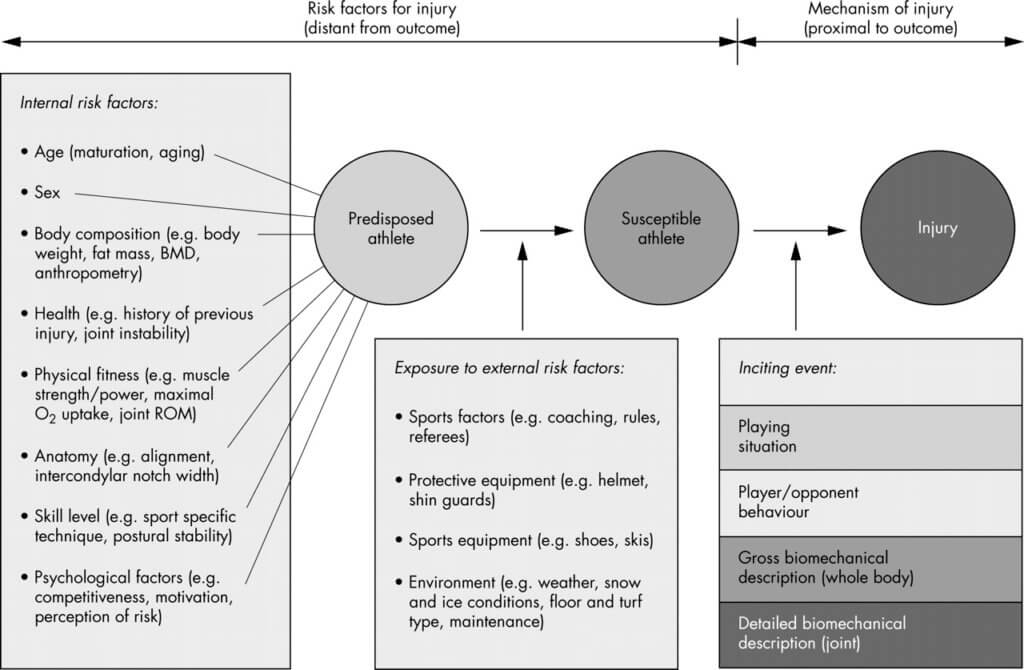
Load management is therefore a major risk factor for injury and tendinopathy. While one would assume absolute high loads are responsible for exceeding tissue capacity resulting in injury, there is evidence to suggest the contrary; absolute high loads actually provide a protective effect in certain sports (7). As such, it currently appears that absolute high loads may not be the problem, rather acute or rapid increases in training load (load spikes) are more likely to put athletes at risk of an injury (7,8). An acute:chronic load concept has been put forward which proposes that if an athlete�s current training load increases by 1.5 + times their previous 4 weeks of training, their risk of injury greatly increases (8).
Redefining How We Describe Lateral Elbow Pain
Lateral elbow tendon pain is a common and frequently occurring work and sport related condition (9). It has often been referred to as �tennis elbow� and diagnosed as �lateral epicondylitis�. The term �epicondylitis� indicates inflammation is the primary cause of tendon pain however, it has since been shown that there is a paucity of inflammation associated with tendon pain, which makes it a redundant term (10). The most appropriate definition is �tendinopathy� which describes persistent tendon pain and impaired function as a result of mechanical loading (10). Therefore, the preferred term to define lateral elbow tendon pain and impaired function associated with mechanical loading is �lateral elbow tendinopathy� (LET) (10).
Prevalence and Presentation of Lateral Elbow Pain
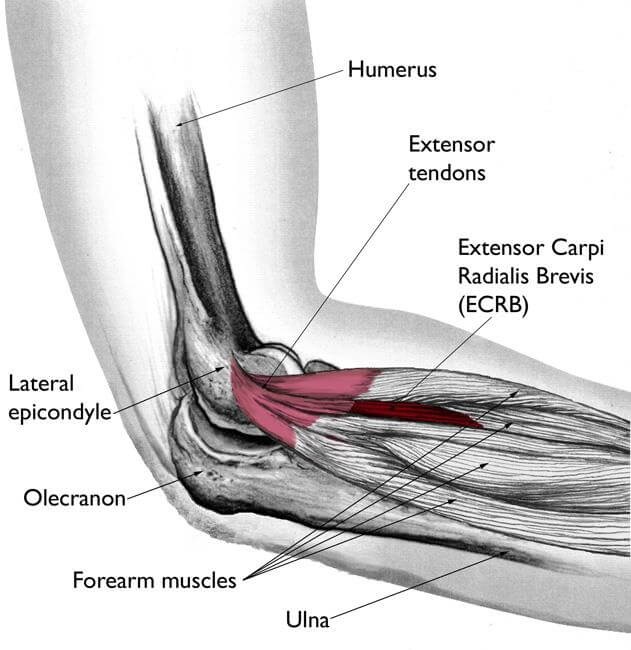
LET is a tendon overload injury that predominantly involves extensor carpi radialis brevis due to overuse of the wrist extensors or supinator (11). It is more common in the dominant arm affecting people between 30-60 years old and it appears to have a longer duration and to be more severe in women (12,13). LET is frequently seen in office workers and athletes yet is seldom seen in tennis players and rarely occurs in elite tennis players (13,14). To read more about the types of elbow pain seen in tennis players you can read Dr. Shannon�s paper on upper limb injuries in elite tennis players.
LET typically involves pain over the lateral elbow that often radiates into the forearm. Pain is brought on by resisted or loading the wrist extensors, there may also be a decrease in grip strength (11,15). Clinical tests include; Cozen�s, Maudsley�s, Mills and grip strength tests (11). Diagnostic imaging should begin with ultrasound, while MRI should be considered if a tear is suspected (15�17).
Treatment of Lateral Elbow Pain
As a tendinopathy, treatment needs to be multimodal focusing on removing and/or managing the excessive loads, correcting any technique or occupational positions resulting in excessive wrist extension and rehabilitating the tendon through mobilization and heavy load based exercises such as, the Cook et.al 4 stage tendinopathy rehabilitation program (1,18�21).
There is inconsistent data on the use of corticosteroid injections; at best they appear to provide only short-term pain relief. This is most likely a reflection of the absence of inflammation associated with tendinopathies (11).
Platelet rich plasma (PRP) injections show better promise for intermediate and longer term pain relief with lower risks of complications (22�24).
Presently there is no strong evidence to support the use of extracorporeal shock wave therapy, laser therapy and transverse friction massage (25�28).
Acupuncture appears at best to provide short term benefit, while therapeutic ultrasound, orthotics and taping require further research to confirm or refute any beneficial outcomes (27,29). The lack of evidence supporting the use of physical therapy interventions would appear to reflect the mechanical load-based nature of tendinopathies.
Final Thoughts on Lateral Elbow Pain
Tendinopathies are notoriously difficult to treat, especially when athletes present in season with one. Patients and athletes have usually been to a myriad of different practitioners and tried unsuccessfully a raft of different treatment interventions. With the right understanding and knowledge of why tendinopathies occur and how best to treat them, chiropractors are well positioned to treat tendinopathies including LET. To further your knowledge and understanding on tendinopathies so you feel confident treating them in your practice; Physiotherapist Ebonie Rio will be presenting on patellar and achilles tendinopathies at the SCA Sports Symposium in Melbourne, May 22-24, 2020. Ebonie is a research fellow at La Trobe University and works with Jill Cook, one of the world�s leading researchers and thinkers in the field of tendinopathies.
If you have lateral elbow pain or any tendon related pain Melbourne city sports chiropractor Dr. Shannon is well placed to help you. Tendinopathy is one of the leading reasons patients present to our CBD sports chiropractic clinic, which we have a high success rate in treating. To book an appointment with Dr. Shannon or to see our sports and remedial massage therapist click on the button below.
References
1. ��������� Cook JL, Purdam CR. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med. 2009 Jun 1;43(6):409�16.
2. ��������� Franchi M, Trir� A, Quaranta M, Orsini E, Ottani V. Collagen structure of tendon relates to function. ScientificWorldJournal. 2007 Mar 30;7:404�20.
3. ��������� Samiric T, Ilic MZ, Handley CJ. Characterisation of proteoglycans and their catabolic products in tendon and explant cultures of tendon. Matrix Biol J Int Soc Matrix Biol. 2004 May;23(2):127�40.
4. ��������� Danielson P, Alfredson H, Forsgren S. Distribution of general (PGP 9.5) and sensory (substance P/CGRP) innervations in the human patellar tendon. Knee Surg Sports Traumatol Arthrosc Off J ESSKA. 2006 Feb;14(2):125�32.
5. ��������� Yu JS, Popp JE, Kaeding CC, Lucas J. Correlation of MR imaging and pathologic findings in athletes undergoing surgery for chronic patellar tendinitis. AJR Am J Roentgenol. 1995 Jul;165(1):115�8.
6. ��������� Kraushaar BS, Nirschl RP. Tendinosis of the elbow (tennis elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am. 1999 Feb;81(2):259�78.
7. ��������� Soligard T, Schwellnus M, Alonso J-M, Bahr R, Clarsen B, Dijkstra HP, et al. How much is too much? (Part 1) International Olympic Committee consensus statement on load in sport and risk of injury. Br J Sports Med. 2016 Sep;50(17):1030�41.
8. ��������� Blanch P, Gabbett TJ. Has the athlete trained enough to return to play safely? The acute:chronic workload ratio permits clinicians to quantify a player�s risk of subsequent injury. Br J Sports Med. 2016 Apr;50(8):471�5.
9. ��������� Stasinopoulos D, Stasinopoulos I. Comparison of effects of eccentric training, eccentric-concentric training, and eccentric-concentric training combined with isometric contraction in the treatment of lateral elbow tendinopathy. J Hand Ther Off J Am Soc Hand Ther. 2017 Mar;30(1):13�9.
10. ������� Scott A, Squier K, Alfredson H, Bahr R, Cook JL, Coombes B, et al. ICON 2019: International Scientific Tendinopathy Symposium Consensus: Clinical Terminology. Br J Sports Med. 2019 Aug 9;bjsports-2019-100885.
11. ������� Ahmad Z, Siddiqui N, Malik SS, Abdus-Samee M, Tytherleigh-Strong G, Rushton N. Lateral epicondylitis: a review of pathology and management. Bone Jt J. 2013 Sep;95-B(9):1158�64.
12. ������� Bisset LM, Vicenzino B. Physiotherapy management of lateral epicondylalgia. J Physiother. 2015 Oct 1;61(4):174�81.
13. ������� Waugh EJ, Jaglal SB, Davis AM, Tomlinson G, Verrier MC. Factors associated with prognosis of lateral epicondylitis after 8 weeks of physical therapy. Arch Phys Med Rehabil. 2004 Feb;85(2):308�18.
14. ������� Descatha A, Albo F, Leclerc A, Carton M, Godeau D, Roquelaure Y, et al. Lateral Epicondylitis and Physical Exposure at Work? A Review of Prospective Studies and Meta-Analysis. Arthritis Care Res. 2016;68(11):1681�7.
15. ������� De Smedt T, de Jong A, Van Leemput W, Lieven D, Van Glabbeek F. Lateral epicondylitis in tennis: update on aetiology, biomechanics and treatment. Br J Sports Med. 2007 Nov;41(11):816�9.
16. ������� Bachta A, Rowicki K, Kisiel B, ?abicka M, Elert-Kope? S, P?omi?ski J, et al. Ultrasonography versus magnetic resonance imaging in detecting and grading common extensor tendon tear in chronic lateral epicondylitis. PloS One. 2017;12(7):e0181828.
17. ������� Latham SK, Smith TO. The diagnostic test accuracy of ultrasound for the detection of lateral epicondylitis: a systematic review and meta-analysis. Orthop Traumatol Surg Res OTSR. 2014 May;100(3):281�6.
18. ������� Cullinane FL, Boocock MG, Trevelyan FC. Is eccentric exercise an effective treatment for lateral epicondylitis? A systematic review. Clin Rehabil. 2014 Jan;28(1):3�19.
19. ������� Hoogvliet P, Randsdorp MS, Dingemanse R, Koes BW, Huisstede BMA. Does effectiveness of exercise therapy and mobilisation techniques offer guidance for the treatment of lateral and medial epicondylitis? A systematic review. Br J Sports Med. 2013 Nov;47(17):1112�9.
20. ������� Rio E, Kidgell D, Moseley GL, Gaida J, Docking S, Purdam C, et al. Tendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative review. Br J Sports Med. 2016 Feb;50(4):209�15.
21. ������� Scott A, Docking S, Vicenzino B, Alfredson H, Zwerver J, Lundgreen K, et al. Sports and exercise-related tendinopathies: a review of selected topical issues by participants of the second International Scientific Tendinopathy Symposium (ISTS) Vancouver 2012. Br J Sports Med. 2013 Jun;47(9):536�44.
22. ������� Coombes BK, Bisset L, Vicenzino B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet Lond Engl. 2010 Nov 20;376(9754):1751�67.
23. ������� Dong W, Goost H, Lin X-B, Burger C, Paul C, Wang Z-L, et al. Injection therapies for lateral epicondylalgia: a systematic review and Bayesian network meta-analysis. Br J Sports Med. 2016 Aug;50(15):900�8.
24. ������� Hussain N, Johal H, Bhandari M. An evidence-based evaluation on the use of platelet rich plasma in orthopedics � a review of the literature. SICOT-J. 2017;3:57. doi:10.1051/sicotj/2017036
25. ������� Capan N, Esmaeilzadeh S, Oral A, Basoglu C, Karan A, Sindel D. Radial Extracorporeal Shock Wave Therapy Is Not More Effective Than Placebo in the Management of Lateral Epicondylitis: A Double-Blind, Randomized, Placebo-Controlled Trial. Am J Phys Med Rehabil. 2016;95(7):495�506.
26. ������� Speed CA, Nichols D, Richards C, Humphreys H, Wies JT, Burnet S, et al. Extracorporeal shock wave therapy for lateral epicondylitis�a double blind randomised controlled trial. J Orthop Res Off Publ Orthop Res Soc. 2002 Sep;20(5):895�8.
27. ������� Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. Br J Sports Med. 2005 Jul 1;39(7):411�22.
28. ������� Loew LM, Brosseau L, Tugwell P, Wells GA, Welch V, Shea B, et al. Deep transverse friction massage for treating lateral elbow or lateral knee tendinitis. Cochrane Database Syst Rev. 2014, Issue 11. Art. No.: CD003528. DOI: 10.1002/14651858.CD003528.pub2
29. ������� Green S, Buchbinder R, Barnsley L, Hall S, White M, Smidt N, et al. Acupuncture for lateral elbow pain. Cochrane Database Syst Rev. 2002, Issue 1. Art. No.: CD003527. DOI: 10.1002/14651858.CD003527
The post Why We Need To Move On From �Lateral Epicondylitis� first appeared on Shannon Clinic.